Allergies
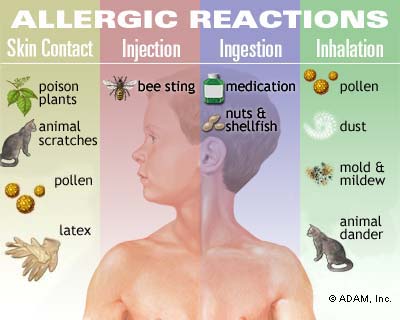
With allergies affecting your skin, respiratory system, and digestion, you should understand common triggers—pollen, dust mites, foods, insect stings, and medications—and how immune responses produce symptoms like rashes, cough, headache, loss of taste or smell, and sore throat. You can identify seasonal versus food or contact allergies, seek ENT evaluation when needed, and consider evidence-informed homeopathic approaches alongside conventional care to manage symptoms and support holistic treatment plans.
The Mechanisms of Allergies
How the Immune System Misfires
You develop an allergic response after your immune system misidentifies a normally harmless protein as a threat, initiating a Type I hypersensitivity cascade driven by IgE. Sensitization begins when antigen-presenting cells present allergen peptides to naïve T cells and skew them toward a Th2 phenotype under the influence of cytokines such as IL-4 and IL-13; those Th2 cells then promote B-cell class switching to IgE. Sensitization can be asymptomatic for weeks to years, but once specific IgE is produced and binds FcεRI receptors on mast cells and basophils, subsequent exposure to the same allergen cross-links the bound IgE and triggers rapid degranulation with the release of histamine, tryptase, leukotrienes, and prostaglandins.
Your clinical symptoms reflect the effector phase: histamine increases vascular permeability and vasodilation, causing hives and angioedema; leukotrienes and prostaglandins produce bronchoconstriction and mucus hypersecretion, causing wheezing and coughing; and chemokines recruit eosinophils that sustain chronic inflammation in tissues such as nasal mucosa or bronchial walls. Anaphylaxis is the systemic extreme of this process, with multiorgan involvement, hypotension and airway compromise; prompt intramuscular epinephrine is the standard emergency treatment. Not all allergies are IgE-mediated, however—you can experience contact dermatitis from T-cell–mediated Type IV reactions (nickel, poison ivy) or immune complex–driven Type III responses in certain drug reactions.
Your susceptibility to these misfires is shaped by genetics, the environment, and prior exposures. Atopy—the inherited tendency to make IgE—is common in populations with positive skin tests in roughly 20–30% of people, and a family history of asthma, eczema, or allergic rhinitis raises your risk considerably. Environmental factors such as early life antibiotic use, urban pollution, and high allergen load in the home (dust mites, pet dander, and mold) bias immune development toward Th2 pathways. Clinical scenarios like food-dependent exercise-induced anaphylaxis, perioperative anaphylaxis to drugs (penicillins, neuromuscular blockers), or severe pollen-triggered asthma illustrate how different triggers converge on the same misdirected immune machinery.
The Role of Allergens in Triggering Responses
Allergens are not all the same; their molecular size, stability, enzymatic activity, and route of exposure determine their sensitizing potential. Proteins that resist digestion and remain intact long enough to interact with immune cells—peanut storage proteins (Ara h family) and shellfish tropomyosin—are notorious for causing systemic food allergies. Inhaled allergens like dust mite (Der p 1 and Der p 2), cat Fel d 1, and pollen allergens such as ragweed Amb a 1 often exist on particles sized 10–40 µm that penetrate the upper and lower airways, while pollen grains themselves range from roughly 10–100 µm and release sub-pollen particles that carry allergenic proteins into your bronchi during high-count days.
The way your skin acts as a barrier and how allergens enter your body affects how likely you are to develop allergies: if your skin is inflamed or damaged, you are more likely to become allergic, which helps explain why certain genetic changes in filaggrin—found in about 10% of people with atopic dermatitis—are connected to higher rates of food allergies and peanut allergies from skin contact.</sent When you breathe in allergens along with environmental factors, it can make your body’s reactions stronger; for example, diesel exhaust particles and other pollutants can help immune cells take in these allergens more easily and increase the chances and seriousness of asthma. Drugs and small molecules like amoxicillin act as haptens, covalently binding to host proteins to create neoantigens that can induce IgE or non-IgE drug hypersensitivity, a mechanism distinct from classical protein allergen pathways.
Your pattern of exposure and the amount you are exposed to are very important: low, repeated exposures often lead to IgE sensitization, while high doses taken orally during infancy can help build tolerance—this is why strategies like introducing peanuts early have been shown in studies to reduce peanut allergy rates. The similarity between related proteins helps explain many clinical cases, such as how being sensitive to birch pollen (Bet v 1) can cause oral allergies syndrome with raw apple or hazelnut, and how people allergic to shellfish may also react to dust mites because of shared trop Occupational exposures—latex in healthcare workers, flour in bakers—demonstrate how sustained high-dose contact substantially increases your risk of developing clinically significant allergies.
Additional mechanistic detail clarifies variability in clinical expression: glycosylation patterns on allergens can engage C-type lectin receptors and modify immune uptake, while proteolytic allergens (Der p 1) actively disrupt epithelial tight junctions, increasing paracellular allergen penetration. Over time, your body’s response to allergens can expand from reacting to just one protein to reacting to many different allergenic components, and things like NSAIDs, alcohol, or exercise can make you more sensitive, turning a mild reaction into a serious anaphylactic reaction in people who are vulnerable.
Identifying Common Allergy Triggers of Allergies
Environmental Allergens: Dust, Pollen, and Mold
If you wake up congested or with itchy eyes every spring, pollen is the likely suspect: tree pollen peaks in early spring, grass pollen in late spring to early summer, and ragweed releases enormous quantities from August through October in the Northern Hemisphere. Local pollen counts, reported as grains per cubic meter, can spike into the thousands on windy days; those spikes correlate tightly with symptomatic flares in allergic rhinitis and conjunctivitis. Checking regional pollen forecasts and noting symptom timing—outdoors after mowing vs. indoors overnight—lets you distinguish tree/grass/ragweed patterns from continuous indoor exposures.
House dust mites, primarily Dermatophagoides pteronyssinus and D. farinae, live in mattresses, pillows, upholstered furniture, and carpets; they proliferate when indoor relative humidity exceeds about 50% and temperatures hover between 20 and 25°C. You may not see them, but you’ll see the consequences: perennial sneezing, nasal congestion, and eczema that worsens at night or after contact with bedding. Objective identification can be aided by home dust mite test kits or by noting symptom improvement after targeted measures—encasing pillows and mattresses in allergen-barrier covers, washing bedding weekly at ≥60°C, and replacing high-pile carpet in bedrooms.
Mold spores act as both seasonal and perennial triggers depending on the species and environment—Alternaria and Cladosporium often spike outdoors in late summer and fall, while indoor molds like Aspergillus and Penicillium persist in damp bathrooms, basements, and areas with water damage. You may notice worsening cough, wheeze, or sinus pressure when humidity rises or after plumbing leaks; air sampling can show colony-forming units per cubic meter that correlate with symptom clusters. Practical identification combines inspection for visible mold, humidity monitoring (aim for <50% indoors), and targeted remediation; failing to correct hidden leaks or condensation keeps mold counts high and symptoms persistent despite medication or avoidance attempts.
Food Allergies: The Usual Suspects and Their Impact

You’ll encounter the eight major food allergens—milk, eggs, fish, shellfish, tree nuts, peanuts, wheat, and soy—most often, since U.S. labeling laws require them to be declared on packaged foods; that legal framework helps you spot obvious culprits. Population studies put food allergy prevalence at roughly 8% in children and between 7 and 10% in adults depending on survey methods, with self-reported rates higher than confirmed cases. Typical reactions range from localized hives and gastrointestinal upset to systemic anaphylaxis; peanuts and tree nuts account for a disproportionate share of severe, life-threatening reactions.
Egg and cow’s milk allergies commonly develop in infancy and are frequently outgrown by school age, while peanut, tree nut, and shellfish allergies more often persist into adulthood. Oral Allergies Syndrome (pollen-food cross-reactivity) produces immediate itching or swelling of the mouth and throat after raw fruits such as apples or bananas if you’re sensitized to birch or grass pollens. Hidden ingredients like MSG, sulfites, or cross-contact in restaurant kitchens can provoke unexpected reactions; if you react despite “safe” choices, trace contamination or mislabeled ingredients are common causes.
If you’ve ever had a delayed reaction—recurrent hives hours after eating or unexplained abdominal pain—you should know that a definitive diagnosis may require skin prick testing, serum-specific IgE tests, and often an oral food challenge under medical supervision. Epinephrine auto-injector prescriptions are indicated for anyone with a history of anaphylaxis or systemic reactions, and food allergy action plans reduce emergency risk at school or work. For persistent or complex cases, referral to an allergist for component-resolved diagnostics or consideration of oral immunotherapy can change long-term risk profiles.
Cross-reactivity patterns are relevant for day-to-day avoidance: for example, if you react to shrimp, you’ll often need to avoid multiple crustacean species rather than a single product, and latex-fruit cross-reactivity can link banana, avocado, and chestnut sensitivities. Careful label reading, carrying epinephrine if you’ve had systemic responses, and maintaining communication with restaurants are practical steps that reduce the chance of inadvertent exposure.
Medication-Induced Allergies: When Prescriptions Backfire
You’ll notice penicillins and sulfonamides near the top of lists for reported drug allergies; about 10% of patients report a penicillin allergy, yet confirmatory testing shows true IgE-mediated penicillin allergy in fewer than 1% of cases. Mislabeling yourself as penicillin-allergic affects treatment choices: clinicians may prescribe broader-spectrum antibiotics such as fluoroquinolones or vancomycin, which increases cost, side effects, and risk of resistant infections and C. difficile. Tracking actual reaction details—timing, rash type, presence of respiratory or cardiovascular symptoms—lets you and your clinician decide whether skin testing or a graded challenge is appropriate.
Reactions to medications split into immediate IgE-mediated responses (urticaria, angioedema, and anaphylaxis within minutes to hours) and delayed T-cell–mediated reactions (morbilliform rashes, fixed drug eruptions, or severe cutaneous adverse reactions such as Stevens-Johnson syndrome and toxic epidermal necrolysis). You may experience a maculopapular rash days after starting a medication like an antibiotic or anticonvulsant; that pattern often signals a delayed hypersensitivity and typically requires stopping the drug and specialist evaluation. For lifesaving therapies where no alternatives exist, supervised desensitization protocols can temporarily induce tolerance under strict medical control.
Cephalosporin cross-reactivity with penicillins is lower than once feared—modern estimates place clinically meaningful cross-reactivity at around 1%—so you won’t always be forced off an entire antibiotic class based on an ambiguous historical label. Documentation in your medical record and carrying an allergy card that specifies the reaction type and date helps emergency and outpatient providers make safer prescribing decisions.
Allergy testing options include skin prick and intradermal tests for quick reactions and patch tests or lymphocyte transformation tests for slower reactions; if a suspected drug allergy could impact your future treatment or limit necessary medications, it’s best to see an allergist-immunologist.
Insect Bites and the Unexpected Reactions
You probably shrug off most mosquito bites as transient itch, but large local reactions—sometimes called Skeeter syndrome—produce pronounced swelling, fever, and secondary cellulitis in children and sensitized adults; those reactions reflect an exaggerated local immune response rather than systemic anaphylaxis. Mosquito saliva contains multiple proteins that act as allergens, and repeated exposures can escalate symptoms over time. If you notice progressive enlargement of a bite over 24–72 hours with warmth and pain, distinguishing allergic swelling from bacterial infection matters for treatment choices.
Stings from bees, wasps, hornets, and fire ants carry a higher risk for systemic anaphylaxis: sudden hives, throat tightness, wheezing, hypotension, or loss of consciousness warrant immediate intramuscular epinephrine and emergency care. Geographic patterns influence risk—fire ant stings are a leading cause of venom-induced reactions in the southeastern United States, while honeybee and yellowjacket stings predominate elsewhere. You should seek allergist evaluation after any systemic sting reaction because venom immunotherapy (VIT) reduces future systemic reaction risk by over 90% in many studies.
Tick bites can create an unusual delayed food allergy known as alpha-gal syndrome: after a bite from the Lone Star tick (Amblyomma americanum), you may develop IgE antibodies to galactose-alpha-1,3-galactose and then experience allergic reactions 3–6 hours after eating red meat. That delayed timing and association with nighttime gastrointestinal distress, plus later hives or anaphylaxis, make the syndrome easy to miss unless you connect the reaction pattern to a recent tick exposure. If you live, work, or recreate in tick-prone areas, noting tick encounters and the timing of delayed symptoms is key to diagnosis.
Carrying an epinephrine auto-injector if you’ve had systemic insect reactions, wearing medical identification, and pursuing venom immunotherapy when indicated are effective strategies to lower future risk; local measures—such as insect-proofing living spaces and using repellents with DEET or permethrin-treated clothing—reduce exposure and the frequency of bite-related allergic events.
Recognizing the Signs of Allergies: Allergy Symptoms Unpacked
Skin Allergies: Rashes, Hives, and Dermatitis
You may first notice an immediate rash after exposure to a trigger—raised, itchy welts (urticaria) that can appear anywhere on your body within minutes of contact with foods, medications like amoxicillin, or insect stings. Acute urticaria affects up to about 20% of people at some point in their lives, and the welts typically blanch when pressed and migrate over hours; when swelling extends into deeper tissues, you get angioedema, which often involves eyelids, lips, or the tongue and can signal a life-threatening airway risk. Chronic urticaria is defined by recurrence beyond six weeks and often lacks an identifiable allergen; autoimmune causes account for a substantial subset, so if your hives are persistent, you should be evaluated for underlying thyroid disease or autoantibodies.
You can also experience contact dermatitis, which presents differently from hives—localized redness, blistering, and scaling where your skin touched nickel, latex, poison ivy, or topical antibiotics. Allergic contact dermatitis is a delayed, T-cell–mediated reaction that typically shows up 24–72 hours after exposure, so the timing helps you distinguish it from immediate IgE-mediated responses; patch testing can identify specific culprits, with nickel and fragrance mixes among the most common positives in clinical series. Atopic dermatitis (eczema) often coexists with food or environmental allergies in children—about 10–20% of kids—but in adults the pattern is more chronic and xerotic, with lichenification and secondary infection risk if you scratch repeatedly.
Red flags in skin reactions include spreading erythema with fever (possible cellulitis), mucosal involvement (Stevens–Johnson spectrum), and any rapid facial or throat swelling that compromises breathing. Case examples illustrate variability—a collegiate swimmer developed urticaria minutes after eating shellfish and required epinephrine, while another patient suffered months of localized hand dermatitis from occupational glove use that resolved only after switching glove materials. Management starts with avoidance of the identified trigger, topical corticosteroids or emollients for dermatitis, and nonsedating antihistamines for urticaria, but recurrent or severe presentations warrant specialist assessment and possible immunologic workup.
Some patients say a commonly prescribed steroid for allergies treatment triggered mania and suicidal ideation.
In a significant number of medical circumstances, the administration of Steroids is required, making it one of the most important treatments that are currently available. Numerous millions of people all over the world are able to avoid death thanks to this medication. I would have to say that insulin, Steroids, and penicillin are the three medicinal drugs that are considered the most significant anywhere in the world.
On the other hand, people frequently use this medication in situations where it is not necessary and doesn’t offer any benefits. The adverse effects of Steroids are the most significant aspect to consider.
It is both reasonable and important from a medical standpoint to prescribe Steroids when they are the sole medication that has the potential to alter the progression of the disease or bring about remission.
However, in many instances, a holistic approach might be significantly more beneficial than steroids, in addition to being safer and more cost-effective.
Even medical disorders that require the use of steroids, regardless of their potential adverse effects, can frequently be treated with a combination of prescription medications, acupuncture, or homeopathic therapies. If this strategy is used, your doctor may give lower steroid doses or omit them from treatment.
Prednisone’s side effects are recognized to have adverse mental health impacts. Still, some patients and doctors claim they can be more severe than most medical professionals realize, especially for such a widely used medication. These prednisone side effects aren’t just “mood swings” but major crises that can cause suicidal thoughts, manic episodes, weeks of insomnia, and hospitalizations for mental illness. Admission to the psychiatric hospital after taking high doses of prednisone is “not an uncommon example of Side effects of prednisone,” according to psychiatrist and suicide epidemiologist Dr. Paul S. Nestadt of Johns Hopkins.
Respiratory Symptoms: Coughing, Sneezing, and Difficulty Breathing
You will commonly experience sneezing fits, clear rhinorrhea, nasal congestion, and itchy eyes during allergic rhinitis episodes; seasonal pollen allergies (hay fever) and perennial triggers like dust mites or pet dander are the usual suspects. Allergic rhinitis affects roughly 10–30% of adults and up to 40% of children, and the classic pattern—worse on waking and during high pollen counts—helps you connect symptoms to environmental exposure. Postnasal drip frequently provokes a nonproductive cough, and persistent cough in the absence of infection should prompt evaluation for upper airway cough syndrome related to allergies.
Asthma and allergic airway inflammation may present with wheeze, chest tightness, and exertional shortness of breath that fluctuates with exposure; about half of people with asthma have allergic triggers that worsen control. Objective testing—spirometry with bronchodilator response or peak expiratory flow variability—can document reversible airflow obstruction and guide management; in clinic, a 20% variability in peak flow across several days is a red flag for poorly controlled allergic asthma. Severe reactions can progress to laryngeal edema or bronchospasm; an episode marked by stridor, inability to speak full sentences, or accessory muscle use requires immediate emergency care.
Patterns help you distinguish seasonal versus perennial causes: seasonal sneezing tied to ragweed or tree pollen contrasts with year-round nasal congestion driven by dust mites or mold in damp homes. Work-related exposures (like wood dust or animal proteins) usually cause symptoms during the week and improve on weekends, which is a helpful sign for diagnosis; allergy tests and steps to control the environment—like using mattress covers, HEPA filters, and fixing mold issues—can significantly lower the frequency of cough and whe Since viral infections, GERD, and side effects from medications (like ACE inhibitors) can look like an allergic cough, paying attention to when symptoms happen and how they respond to antihistamines or inhaled
A more thorough evaluation involves checking peak flow rates during times of high exposure and measuring exhaled nitric oxide to assess inflammation in the airways; high levels of fractional exhaled nitric oxide (FeNO) often indicate that steroids will be effective for Symptom diaries that track pollen counts, indoor humidity, and exposure to pets can reveal triggers you can mitigate. If you lose taste or smell alongside nasal obstruction, consider severe congestion or referral testing, since persistent anosmia merits ENT evaluation for sinonasal disease or other causes.
Gastrointestinal Distress: Nausea and Digestive Issues
You can experience GI symptoms from immune-mediated food allergies that range from mild oral tingling and nausea to vomiting and diarrhea within minutes to a few hours after ingestion; oral allergy syndrome—itching of the mouth and throat after eating raw fruits like apples or bananas—is common in people with pollen sensitization due to cross-reactive proteins. Food allergies affect about 8% of children and roughly 4% of adults, with milk, egg, peanut, tree nuts, soy, wheat, fish, and shellfish accounting for the majority of cases; in children under two, milk and egg allergies are particularly prevalent. Severe GI presentations may accompany systemic reactions—if you have simultaneous vomiting, abdominal pain, urticaria, or respiratory compromise after eating, consider the possibility of anaphylaxis.

Eosinophilic gastrointestinal disorders present another pattern: chronic abdominal pain, refractory reflux, or dysphagia that correlates to specific food triggers and shows eosinophil-predominant inflammation on endoscopic biopsy. Food protein-induced enterocolitis syndrome (FPIES) is a non-IgE-mediated reaction seen in infants and young children, characterized by repetitive, projectile vomiting and lethargy 1–4 hours after ingestion of triggers such as cow’s milk or soy. Distinguishing true food allergy from intolerances—lactose malabsorption, celiac disease, or irritable bowel syndrome—is crucial, since only immune-mediated allergies carry immediate anaphylaxis risk and require strict avoidance and an emergency action plan.
Diagnostic approaches that help you pinpoint allergy-related GI symptoms include targeted skin or serum IgE testing, supervised oral food challenges, and endoscopy with biopsy when eosinophilic pathology is suspected. Timing of symptom onset is a valuable clue:IgE-mediated reactions typically begin within minutes to two hours, while delayed cell-mediated responses can appear over several hours to days. If you have recurrent GI complaints tied to certain meals, keeping a detailed food-symptom log and seeking evaluation by an allergist or gastroenterologist can prevent mislabeling and guide appropriate dietary management.
Gastrointestinal symptoms often happen along with skin or breathing problems during serious reactions—research shows that vomiting occurs in 30–70% of children with anaphylaxis, depending on what caused it—so if you only have stomach issues after eating a risky food, it’s still important to Cross-reactivity examples help you anticipate triggers: patients with birch pollen allergy frequently react to raw apple due to similar profilins, while shellfish allergy tends to produce more severe systemic symptoms in adults. Understanding these patterns helps you and your clinician plan diagnostic oral challenges or elimination diets safely.
Neurological Responses: Headaches and Cognitive Effects
You may notice headaches, migraine exacerbations, or a persistent “brain fog” during allergy flares, with sinus congestion and pressure commonly producing frontal or facial pain that mimics tension-type headaches. Histamine and other inflammatory mediators released during allergic reactions can influence cerebral vasodilation and nociceptive pathways, and some patients report that antihistamine-responsive headaches coincide with peak pollen seasons. In cohort surveys, a significant proportion of people with allergic rhinitis—estimates vary but often exceed 30%—report concurrent headache or migraine worsening during symptomatic periods.
Sleep disruption from nocturnal nasal obstruction or coughing creates secondary cognitive impairment: daytime sleepiness, reduced concentration, and impaired memory performance that can be objectively measured on attention tasks. Children with uncontrolled allergic rhinitis or asthma show higher rates of school absenteeism and impaired academic performance; treating the underlying allergic disease frequently leads to measurable gains in attention and reduced behavioral complaints. Sensitivity to dietary triggers such as monosodium glutamate (MSG), sulfites, or aged cheeses can precipitate migraine in susceptible individuals, so correlating dietary intake with headache patterns is a practical diagnostic step.
Chronic neuroinflammatory signaling may amplify preexisting headache disorders; if you have cyclic migraine attacks that align with environmental exposures or menstrual cycles, consider allergy as a modifiable trigger that, when controlled, often reduces frequency and severity. Neurocognitive symptoms also appear in the context of systemic allergic reactions—cytokine surges can produce malaise and slowed processing speed that resolve once inflammation subsides. For persistent or severe neurological complaints associated with allergy, coordinated care involving allergy and neurology specialists helps differentiate primary neurologic disease from allergy-driven symptoms.
More detailed patterns include morning-predominant headaches tied to nocturnal nasal congestion and postnasal drip, as well as cognitive slowing that improves after effective nasal steroid therapy or allergen avoidance. Documenting symptom timing, sleep quality, and response to allergy medications provides actionable data for your clinician to tailor treatment that reduces both headache burden and cognitive impact.
Seasonal Struggles: How Allergies Change with the Seasons
Spring Awakenings: The Pollen Predicament

When tree pollen peaks in March through May in many temperate zones, you often feel it first: itchy eyes, repeated sneezing, and that scratchy throat that makes you reach for tissues every class or commute. Specific offenders include birch, oak, maple and alder, with regional differences—for example, cedar blooms in the Southwest earlier and can trigger severe symptoms in otherwise low-pollen months. You can monitor local pollen forecasts to time outdoor exposure; pollen counts are measured as grains per cubic meter and can surge by hundreds or thousands on windy, dry days, so a high-count morning might explain why your run through the park leaves you congested for the afternoon.
Exposure patterns matter: grass pollen, which usually follows tree pollen and peaks from late spring into early summer, tends to be highest in suburban lawns and sports fields, so if you coach or mow your lawn, you may be exposed to higher concentrations than people in dense urban centers. A 2018 clinic series showed patients with seasonal allergic rhinitis had markedly worse quality-of-life scores during peak tree and grass pollen weeks, with sleep disruption and concentration problems reported by 40–60% of respondents. You can track specific plant calendars—in much of North America, oak and birch dominate March–April, and grasses dominate May–July—to anticipate which symptoms may flare.
Symptoms can vary by exposure route and dose: breathing small pollen-laden aerosols produces sneezing, clear rhinorrhea, and itchy conjunctiva, while heavier exposures can provoke tightness in the chest for people with asthma. Cross-reactivity is common; you may notice oral itching with raw apples, carrots or celery if you react to birch pollen (oral allergy syndrome), which explains why antihistamines alone sometimes leave residual mouth or throat prickling. If you live near high-pollen corridors—highways lined with ornamental grasses or riparian zones with alder stands—consider timed avoidance, washing hair and clothes after outdoor work, and indoor air strategies such as running a portable HEPA filter that captures ~99.97% of particles down to 0.3 microns to reduce symptom burden indoors.
Summer’s Hidden Hazard: Mold Growth
Warmth plus humidity creates fertile conditions for outdoor and indoor molds; outdoor spore counts commonly rise in late summer after heat spells and thunderstorms, and you may notice sneezing and post-nasal drip that mimic hay fever but persist into evenings when you return indoors. Basements, crawl spaces, and poorly maintained HVAC systems are frequent indoor reservoirs where Aspergillus, Cladosporium and Alternaria proliferate; a home inspection series found visible mold or water damage in roughly 20–30% of older houses, and you are far more likely to flare if you sleep near a damp basement wall or use a swamp cooler. Sensitization to mold often shows up as chronic cough, wheeze, and persistent sinus congestion rather than the intense eye itch of pollen, so mold-driven symptoms can be mistaken for recurrent sinus infection unless you look for damp spots and musty odors.
Exposure assessments matter because mold spores are measured in spores per cubic meter and outdoor counts can reach the thousands after rainy weeks, especially where leaf litter and compost piles are common; if you volunteer at a community garden or handle mulch, you may experience significant exposure events. You can reduce risk by controlling indoor humidity (aiming for 40–50%), fixing leaks promptly, and keeping exhaust fans running in bathrooms and kitchens during and after use. Case reports show that remediation of visible mold and reduction of indoor humidity often lead to measurable drops in symptom scores over 4–8 weeks in sensitized individuals, so environmental fixes can be as impactful as medications for many people.
Extra detail: if you have a history of asthma, summer mold spikes can precipitate exacerbations—clinical surveillance studies indicate that emergency department visits for asthma rise following heavy summertime rainfalls in humid regions, likely because storms stir large volumes of fungal spores and fragments; you should heed local weather alerts and consider stepping up controller therapy or carrying rescue medication during high-spore intervals.
Fall Allergies: Ragweed and Other Culprits
Ragweed becomes the dominant airborne allergen from late August through November in much of North America, and one ragweed plant can produce up to one billion pollen grains per season, explaining why even small patches along roadsides can create widespread problems. You may notice classic symptoms—sneezing, clear nasal discharge, and itchy eyes—but fall exposures often compound with elevated mold spores from harvested fields and leaf litter, producing prolonged congestion and fatigue that lasts beyond a single pollen peak. Travel or relocation in fall can be revealing: people who move from coastal to inland areas frequently report an uptick in symptoms when they encounter ragweed-dense environments they previously avoided.
Food cross-reactions are relevant in fall: if you react to ragweed pollen you might experience oral allergy syndrome with melons, bananas or cucumbers, producing tingling or swelling in the mouth after eating raw fruit. Agricultural activities increase your exposure; harvesting, composting and leaf-blowing aerosolize both pollen and fungal spores, and occupational studies among landscapers and farmworkers show higher rates of rhinitis and work-related asthma during peak fall seasons. Monitoring ragweed maps and scheduling outdoor chores for low-wind, overcast days can materially reduce your exposure, since pollen dispersal is greatest on sunny, breezy afternoons.
Local control can be effective: targeted removal of ragweed near homes and schools (within a 150–300 meter radius) reduces neighborhood pollen loads and has been associated with fewer symptom-days in some population studies, though eradication is impractical over large areas. You should combine personal measures—showering after outdoor work, changing clothes, and drying laundry indoors during peak ragweed weeks—with community-level interventions like timed mowing and municipal weed control to lower collective exposure and symptom frequency.
Extra detail: fall allergen patterns vary with climate shifts—milder autumns and late frosts extend ragweed pollen seasons by several weeks in some temperate zones, so your historical expectations for symptom timing may not hold; consult multi-year pollen trend data from your local allergy clinic or national monitoring network to plan interventions and medication timing more precisely.
Winter Woes: Indoor Triggers and Dry Air Effects
Closed windows and continuous heating trap indoor allergens and concentrate them around you during winter; pet dander, dust mite fecal particles, and cockroach allergens become dominant triggers while outdoor pollen typically drops. You may notice increased nasal crusting, dry cough, and more frequent nosebleeds due to mucosal drying at relative humidities below 30%. Keeping humidity in the 40–50% range reduces mucosal irritation and dust mite activity, but if you over-humidify, you risk encouraging mold and dust mite proliferation, so you should use a reliable hygrometer to guide adjustments rather than guessing.
Heating systems and fireplaces contribute particulates and combustion byproducts that can mimic or worsen allergy symptoms; studies comparing symptom diaries of patients with perennial rhinitis show spikes in symptom severity during heating season, particularly on days when indoor particulate levels increase. You can lower particulate and allergen load by replacing furnace filters with MERV-rated or HEPA options where compatible, vacuuming with HEPA-equipped cleaners, and washing bedding weekly at 130°F (54°C) if possible to kill dust mites. Year-round allergen sensitization becomes clearer in winter because seasonal pollen exposure is minimal, so if your symptoms worsen indoors, you should test for perennial triggers like dust mites and pet dander.
Dry air also alters mucus properties and innate airway defenses: studies demonstrate that airway surface liquid viscosity increases in low-humidity environments, impairing ciliary clearance and making you more prone to secondary infections and prolonged cough after allergen exposure. Using room humidifiers set to 40–50%, applying saline nasal sprays to maintain mucosal moisture, and avoiding direct heaters aimed at your face can reduce irritation and improve sleep quality during the winter months.
Extra detail: holiday travel and indoor crowding raise viral exposure and can complicate diagnosis—if you develop fever, green sputum, or systemic symptoms, you may have an infection rather than an allergy; conversely, persistent clear watery rhinorrhea with itchy eyes across weeks of indoor living is more consistent with perennial allergic triggers, so documenting symptom timing relative to travel, gatherings, and changes in indoor humidity helps your clinician distinguish causes and tailor interventions.
The Unseen Consequences: Long-Term Effects of Allergies
Chronic Conditions Linked to Allergies
Allergic inflammation frequently evolves beyond intermittent sneezes or itchy eyes and becomes a driver of persistent respiratory disease; asthma now affects roughly 339 million people worldwide and allergic sensitization accounts for a large share of pediatric asthma—studies report sensitization in as many as 60–80% of children with asthma. Repeated exposure to triggers such as dust mites, ragweed, pet dander, or mold can remodel airway architecture over years, increasing bronchial hyperresponsiveness and reducing baseline lung function. You can see this clinically when patients with long-standing allergic rhinitis progress to persistent asthma, requiring inhaled corticosteroids and more frequent rescue therapy, and in cohort data showing higher rates of emergency visits among those with uncontrolled allergic disease.
Upper airway disease becomes chronic for many: allergic rhinitis, affecting roughly 10–30% of the global population, often coexists with chronic rhinosinusitis, and a subset—estimated at 20–30% in some clinics—develops nasal polyps driven by type 2 inflammation. Eosinophilic esophagitis (EoE) has risen in recognition over the past two decades and is now commonly encountered in patients with multiple atopic conditions and food-triggered symptoms; you may notice progressive dysphagia, food impaction, or strictures in patients whose food allergies went untreated. Persistent skin involvement—atopic dermatitis and chronic urticaria—also follows allergic sensitization, with atopic dermatitis affecting 15–20% of children and often extending into adult life for a substantial minority, leaving you to manage xerosis, lichenification, and secondary infections over years rather than weeks.
Systemic consequences accumulate as allergic inflammation disrupts sleep and productivity and fosters comorbidities: chronic nasal congestion predisposes to sinus infections and eustachian tube dysfunction, while untreated allergic asthma increases the risk of exacerbations and hospitalizations—emergency department visits for asthma exacerbations number in the hundreds of thousands annually in large health systems. Long-term steroid use for poorly controlled allergic disease carries metabolic and bone-density risks, and ongoing inflammation can amplify susceptibility to secondary bacterial infections in the sinuses and lower airways. You should therefore consider allergies as potential contributors to multi-organ chronic disease rather than isolated episodic symptoms and plan long-term management accordingly.
Mental Health Implications: Anxiety and Depression
Chronic allergic diseases significantly impact mental health by causing disrupted sleep, persistent discomfort, and social limitations; studies show that individuals with allergic rhinitis, chronic urticaria, or severe food allergies experience higher rates of depressive and anxiety symptoms, with several large cohorts indicating a 20–50% increased prevalence of mood symptoms compared to those without allergies. Nighttime nasal obstruction and coughing fragment sleep architecture, leading to daytime fatigue, impaired concentration, and lowered resilience—factors that compound vulnerability to anxiety disorders. You can observe this pattern when patients with severe perennial allergies describe declining work performance and heightened worry during high-pollen seasons or before social events that involve food.
Biological mechanisms also link allergy and mood: chronic type 2 inflammation releases cytokines (IL-4, IL-5, and IL-13) and mediators that interact with central nervous system pathways, and systemic inflammation has been associated with altered neurotransmitter metabolism in other inflammatory diseases. Behavioral consequences add further strain—avoidance of social situations due to food allergy risk or visible skin flares increases isolation, and the unpredictability of anaphylaxis can create persistent hypervigilance. In clinical practice you may find that treating the allergic inflammation (for example, improved control of rhinitis or eczema) reduces depressive symptoms and improves sleep, supporting an integrated approach that addresses both physical and psychological domains.
Screening for mood disorders should be part of long-term allergy care because combined management improves outcomes: brief validated tools like the PHQ-9 for depression and GAD-7 for anxiety fit easily into allergy clinics, and collaborative care models—linking allergists with mental health professionals—have demonstrated improvements in adherence, symptom burden, and quality-of-life scores on instruments such as the RQLQ and SF-36. You can take practical steps like improving sleep habits, reducing nighttime nasal blockage with specific treatments (like intranasal corticosteroids, saline rinses, and avoiding allergens), and making quick referrals for cognitive-behavioral therapy or mental health evaluations if screening shows moderate to severe mood issues.
How to Diagnose Your Allergies: Tests and Techniques
Skin Prick Tests: What to Expect
During a skin prick test a technician places small drops of standardized allergen extracts—common panels include dust mite (Der p and Der f), ragweed, grass pollens, cat dander (Fel d 1), and food extracts like peanut or egg—along a row on your forearm or back and pricks the skin through each drop with a sterile lancet. A histamine control and a saline (negative) control are used to check skin responsiveness and technique; the test is read after roughly 15–20 minutes when wheal-and-flare reactions peak. Labs and clinics usually consider a wheal diameter at least 3 mm larger than the saline control as a positive reaction, and technicians will measure both the wheal and the surrounding flare to document the size precisely in millimeters for your record.
Clinicians interpret skin prick results in the context of your history: a 6–8 mm wheal to dust mite correlates strongly with perennial rhinitis and asthma in a patient who reports year-round nasal congestion, while a small 2–3 mm wheal to peanut in someone who has never had oral symptoms is often considered sensitization without proven clinical allergy. Medications and skin conditions change test accuracy—antihistamines blunt results (you may be asked to stop nonsteroidal antihistamines 48–72 hours before testing), and extensive eczema or dermatographism can make interpretation difficult. Cross-reactivity can also produce positive tests to botanically related allergens (for example, birch pollen can cause oral allergy syndrome with apple or hazelnut), so positive skin tests do not always mean you will have clinical reactions to every positive extract.
Expect minor local itching and redness as the most common immediate effects; systemic reactions are rare but clinics that perform skin testing keep epinephrine and resuscitation equipment available as a safety measure. Testing is cost‑effective and gives rapid results, which makes it the preferred first-line diagnostic for inhalant allergies such as pollen, dust mites, and animal dander when you are not taking interfering medications and do not have skin disease that would invalidate the results. Results should guide further steps—if your history and skin test disagree, your clinician may order blood tests or plan supervised food or drug challenges to confirm clinical allergy.
Blood Tests: Measuring Immunoglobulin E Levels
You may be offered blood testing for specific IgE (sIgE) when skin testing is contraindicated—examples include ongoing antihistamine use that cannot be stopped, extensive eczema, pregnancy, or use of beta‑blockers that would complicate emergency treatment of a systemic reaction. Laboratories report sIgE in kilo units per liter (kU/L) and many use 0.35 kU/L as the lower limit of detection; total IgE is reported in international units per milliliter (IU/mL) and can be elevated with atopy but is not diagnostic by itself. Results typically return in 24–72 hours, which makes blood testing useful when you need diagnostic information without pausing chronic medications or waiting for a skin‑test appointment.
Interpretation of sIgE values requires nuance: higher numbers generally increase the probability of clinical reactivity but do not perfectly predict severity on exposure. For certain allergens clinicians use age‑specific decision points—some pediatric guidelines indicate that a peanut sIgE above particular lab-validated thresholds corresponds with a high positive predictive value for clinical allergy, whereas low but detectable sIgE (e.g., 0.35–2 kU/L) often warrants correlation with your symptoms or an oral challenge. Component‑resolved diagnostics (CRD) refine risk assessment by identifying responses to specific proteins, for example, Ara h 2 in peanut allergy, which has a stronger association with systemic reactions than sensitization to cross‑reactive components; CRD requires discussion with your allergist about clinical utility and cost.
Blood tests avoid false negatives due to antihistamines and are preferable when skin testing is impractical, but they can pick up clinically irrelevant sensitization—positive sIgE without symptoms is common, particularly to foods and cross‑reactive pollens. Your clinician will combine sIgE results with detailed exposure history, symptom patterns (such as seasonal vs. perennial rhinitis, exercise‑related anaphylaxis, or reproducible gastrointestinal symptoms after milk or egg), and, when necessary, challenge testing to reach a diagnosis rather than relying on a single laboratory value.
More information: the labs that perform sIgE and total IgE assays vary in methodology and reference ranges, so direct comparison of absolute numbers between different laboratories can be misleading; your allergist will interpret results using the specific lab’s reference intervals and may use likelihood ratios or validated decision points for common allergens such as peanut, egg, milk, and tree nuts. Component testing names you may see include Ara h 1/2/3 for peanut, Bos d 8 for cow’s milk casein, Gal d 1 for egg white, Fel d 1 for cat, and Der p 1/Der p 2 for dust mite; identifying sensitization to a stable, heat‑resistant protein often raises concern for systemic reactions, whereas sensitization limited to labile proteins suggests milder oral symptoms like those in oral allergy syndrome.
Oral Food Challenges: Assessing Food Allergies
Oral food challenges are the diagnostic gold standard for food allergy and are performed under direct medical supervision because they reproduce the reaction in a controlled setting. Challenges range from open (clinician and patient know the food) to single‑blind or double‑blind placebo‑controlled food challenges (DBPCFC), with DBPCFCs most often used in research or when subjective symptoms and anxiety may confound results. The protocol typically uses incremental dosing every 15–30 minutes starting from a tiny amount—often milligrams—and progressing through a planned sequence until a target cumulative dose approximating a normal serving size is reached, while clinicians watch for objective signs such as hives, vomiting, wheezing, or hypotension.
Indications include unclear history despite positive skin or blood tests, verifying resolution of childhood allergies (many children outgrow cow’s milk and eggs by school age), and confirming that avoidance is necessary before imposing lifelong dietary restrictions. Many allergy clinics will perform a supervised baked‑milk or baked‑egg challenge when sIgE and clinical history suggest possible tolerance to heat‑denatured proteins, because tolerance to baked forms often predicts a milder natural history. Preparation often includes withholding antihistamines for a period before the challenge and ensuring that asthma is well controlled, since uncontrolled respiratory disease raises the risk of severe reactions.
Risks of oral food challenges include hives, vomiting, wheezing, or anaphylaxis, so the setting must have immediate access to intramuscular epinephrine, oxygen, and monitoring; standard emergency dosing for epinephrine in anaphylaxis typically follows 0.01 mg/kg up to 0.3–0.5 mg intramuscularly, but clinicians tailor treatment to body weight and response. Observation after a reaction extends for at least a few hours to detect biphasic responses, and some clinics will provide a written emergency plan and prescription for an epinephrine auto‑injector at discharge. Because false positives can arise from anxiety or taste‑related symptoms, the double‑blind approach reduces bias but requires food masking and pharmacy support, making it less available outside specialized centers.
More information:double‑blind placebo‑controlled food challenges reduce subjective reporting and are the standard in clinical trials, while open challenges are commonly used in routine practice where the pretest probability is high or low and the logistics of DBPCFC are impractical. Typical challenge schedules escalate doses roughly exponentially (for example, 1 mg → 3 mg → 10 mg → 30 mg → 100 mg → 300 mg → 1000 mg), aiming to reach an age‑appropriate serving, and clinics document both objective signs and patient‑reported symptoms to decide when to stop the challenge and initiate treatment.
Antihistamines and Decongestants: The First Line of Defense
You can expect antihistamines to blunt the histamine-driven triad of sneezing, itching, and rhinorrhea within minutes to a few hours, depending on the agent. Second‑generation oral antihistamines—cetirizine (commonly 10 mg once daily), loratadine (10 mg once daily), and fexofenadine (60 mg twice daily or 180 mg once daily)—offer effective symptom control with minimal sedation compared with first‑generation drugs like diphenhydramine, which still causes drowsiness and anticholinergic effects. Intranasal antihistamines such as azelastine produce faster relief of nasal symptoms, often within 15–30 minutes, and can be particularly helpful if nasal congestion and ocular symptoms coexist. Pediatric dosing follows age bands (for example, cetirizine 2.5–5 mg daily in young children), so check product labels or consult your clinician for weight‑based recommendations.
Decongestants provide short‑term relief of nasal obstruction but carry important limitations you should weigh. Oral pseudoephedrine works within 30–60 minutes (typical dosing is 60 mg every 4–6 hours, maximum 240 mg/day) and can raise blood pressure and heart rate, so avoid it if you have uncontrolled hypertension, ischemic heart disease, or severe anxiety. Topical nasal decongestants like oxymetazoline give powerful vasoconstriction and fast relief, but using them more than 3–5 consecutive days commonly produces rebound congestion (rhinitis medicamentosa). Combining an oral or intranasal antihistamine with an intranasal steroid often controls both itch/sneeze and congestion better than either alone, and this combination strategy is reflected in many guideline algorithms for allergic rhinitis management.
Side effects and interactions should direct your choice of agent: alcohol and other sedating drugs amplify first‑generation antihistamine drowsiness, while anticholinergic effects (dry mouth, urinary retention) make those agents less suitable for older adults. If you have comorbid asthma, allergic conjunctivitis, or chronic sinusitis, target therapy accordingly—add an intranasal steroid or ocular antihistamine drops rather than escalating systemic antihistamines. For short, acute flares, you may use higher‑potency or sedating agents at night to aid sleep; for daily seasonal or perennial control, second‑generation, non‑sedating antihistamines are generally preferred because they preserve cognition and work/school performance.
Corticosteroids: Reducing Inflammation and Symptoms
Intranasal corticosteroids are the most consistently effective medications for allergic rhinitis, suppressing the underlying mucosal inflammation that drives symptoms. Products like fluticasone propionate (50 mcg per spray, typical regimen: 1–2 sprays per nostril once daily), mometasone (50 mcg per spray), and budesonide have an onset of measurable benefit within 24 hours for some patients, with a maximal effect over 1–2 weeks. You should expect reductions in nasal congestion, rhinorrhea, sneezing, and ocular itching; in randomized trials these sprays outperform antihistamines for congestion relief and overall symptom control. Local adverse effects are generally mild—nasal dryness, burning, or occasional epistaxis—and serious systemic effects such as adrenal suppression are rare at recommended intranasal doses.
For lower respiratory allergic inflammation, inhaled corticosteroids (ICS) such as budesonide or fluticasone are cornerstone therapy in asthma management, reducing exacerbations and airway hyperreactivity when used regularly. Typical adult ICS dosing varies by drug and device, for example budesonide 200–400 mcg twice daily in moderate disease, adjusted by severity and combined with long‑acting bronchodilators as needed. Short courses of systemic oral corticosteroids (prednisone 40–60 mg daily for 3–7 days) remain indicated for severe exacerbations of asthma or angioedema where rapid suppression is necessary, but these carry well‑known systemic risks—hyperglycemia, mood changes, sleep disturbance, and immunosuppression—so you and your clinician should use the lowest effective dose for the shortest duration.
Topical corticosteroids for skin allergies follow potency and site‑specific rules: low‑potency agents (hydrocortisone 1%) suit the face and intertriginous zones, while medium‑to‑high potency steroids manage lichenified eczema or severe contact dermatitis for limited periods. Prolonged use of potent topical steroids can cause skin atrophy, telangiectasia, and striae; children are more susceptible to systemic absorption and growth effects. For chronic allergic skin disease, step‑down strategies, intermittent maintenance schedules, and steroid‑sparing agents such as calcineurin inhibitors can help you maintain control while minimizing steroid exposure.
Using corticosteroids along with other treatments usually leads to better results: using intranasal steroids with oral antihistamines helps reduce both nasal and eye symptoms more than using either one by itself, and using a spacer with inhaled steroids helps the medicine reach the lungs better and reduces side effects If you are pregnant or planning pregnancy, budesonide has the most safety data for inhaled use, and most intranasal steroids are considered acceptable after discussion with your provider. Monitor blood glucose if you require repeated systemic steroid bursts, and coordinate with your primary care or endocrinology team if you have diabetes or risk factors for steroid‑related complications.
Immunotherapy: The Long Game of Desensitization
Allergen immunotherapy alters disease trajectory by inducing immune tolerance rather than merely masking symptoms. Subcutaneous immunotherapy (SCIT) follows a buildup phase—weekly injections with escalating allergen concentration over 3–6 months—then a maintenance phase of injections every 4 weeks for approximately 3–5 years. Patients with moderate‑to‑severe allergic rhinitis or venom allergy who adhere to a full course frequently experience durable reductions in symptom and medication scores, and several studies report sustained benefit for years after stopping therapy. You must undergo skin or specific IgE testing to identify target allergens before starting, and SCIT requires administration in a clinic with a 30‑minute post‑injection observation period because systemic reactions, including anaphylaxis, are uncommon but possible.
Sublingual immunotherapy (SLIT) offers a convenient at‑home alternative for certain allergens such as grass, ragweed, and house dust mites; you typically start the tablet or drop under supervision and then continue daily, with treatment durations of 3 years recommended for sustained benefit. Local oral side effects—tingling or itching under the tongue—occur in up to 40% of users but usually resolve within days to weeks; systemic reactions are rare but possible, and guidelines advise avoidance in uncontrolled asthma. Cost and insurance coverage vary considerably: SCIT often requires clinic visits but may be covered as a medical benefit, whereas SLIT may be a pharmacy expense; discuss logistics and cost‑benefit with your payer and allergist before committing.
Patient selection matters: immunotherapy is most effective for well‑defined, clinically relevant IgE‑mediated allergies where avoidance and pharmacotherapy fail to provide adequate control or where you want to reduce long‑term medication dependence. For example, someone with a perennial dust‑mite allergy who remains symptomatic on intranasal steroids and antihistamines may halve their medication use after 2–3 years of immunotherapy and experience fewer exacerbations of allergic asthma. Contraindications include severe or uncontrolled asthma and certain immunologic disorders; age limits vary by product, but many SLIT tablets are approved for children as young as 5–12 depending on the allergen.
Practical considerations frequently determine whether you pursue immunotherapy: expect a 3–5 year commitment, regular follow‑ups, and upfront costs that may be offset over time by reduced medication and fewer clinic visits for exacerbations. If you travel frequently or cannot attend regular clinic appointments, SLIT’s daily at‑home dosing can be more practical, while SCIT remains the gold standard for multi‑allergen sensitivity and venom immunotherapy. Discuss baseline pulmonary function testing, emergency action plans (including access to epinephrine), and documented outcomes tracking with your allergist before initiating therapy so you can weigh efficacy, safety, and lifestyle fit.
Exploring the Holistic Approach to Allergy Management
Dietary Changes: Foods That Help and Harm
Incorporate anti-inflammatory and immune-supporting foods such as oily fish (salmon, mackerel, sardines) twice weekly to supply long-chain omega-3s, and add ground flaxseed or chia (1–2 tablespoons daily) if you don’t eat fish. Pack each day with vitamin C–rich choices—orange, kiwi, red bell pepper—to help stabilize mast cells; the recommended daily intake is roughly 75 mg for women and 90 mg for men, which you can meet through one medium orange plus a cup of bell pepper slices. Focus on flavonoid-containing foods like apples, onions, parsley and capers for natural quercetin sources that have been associated with reduced histamine release in some observational studies, and aim for at least five servings of vegetables and two servings of fruit per day to maintain a broad micronutrient profile that supports immune balance.
Probiotic and prebiotic strategies can change the way your immune system reacts to allergens. Include one serving daily of fermented foods such as plain yogurt with live cultures, kefir, or kimchi, and augment with prebiotic vegetables—garlic, leeks, asparagus, and bananas—to feed beneficial gut bacteria. If you consider supplements, look for evidence-backed strains like Lactobacillus rhamnosus GG or Bifidobacterium species used in clinical trials; discuss dose and strain with a clinician so you get a product appropriate for your needs. Avoid habitual high-sugar intake and ultra-processed foods, since diets with excessive refined carbohydrates have been correlated with greater systemic inflammation and can worsen subjective allergy symptoms such as nasal congestion and throat irritation.
Elimination strategies should be specific to your clinical pattern: for suspected IgE-mediated reactions to dairy, egg, peanuts, tree nuts, shellfish, soy or wheat, pursue testing and supervised challenges rather than ad hoc removal. For non-IgE sensitivities or suspected histamine intolerance, try a low-histamine diet (avoiding aged cheeses, smoked meats, fermented products, certain fish like tuna and mackerel, and alcohol) for 2–6 weeks while tracking symptom changes; note that sulfite-containing foods and drinks (dried fruits, some wines, and shrimp preservative labels E220–E228) can provoke asthma in roughly 5–10% of people with asthma, so check labels carefully. Practical habits include reading ingredient lists for hidden MSG and sulfites, choosing whole foods over processed alternatives, and consulting a registered dietitian for structured reintroduction to identify true triggers without nutritional compromise.
Lifestyle Modifications: Environmental Controls
Treat the bedroom as your primary allergy-management zone: encase mattresses and pillows in allergen-impermeable covers, wash bedding weekly in water at 54°C (130°F) to inactivate dust mites, and remove wall-to-wall carpeting if possible since carpets can harbor dust mite and mold reservoirs. Maintain indoor relative humidity between 30% and 50%—dust mites proliferate above 50% and many molds thrive when humidity stays elevated—by using dehumidifiers or HVAC systems with humidity controls. Invest in a high-efficiency vacuum with a sealed HEPA filter and run it at least twice weekly in allergen-prone areas; change HVAC filters every 1–3 months and consider MERV 11–13 filters or standalone HEPA air purifiers sized to the room’s square footage (match CADR to room size; for example, a 150 sq ft bedroom typically needs a CADR ≥150).
Outdoor-trigger management reduces seasonal and pollen-related flares: check local pollen forecasts and limit outdoor activity during peak pollen times, which often occur in the early morning and on dry, windy days; switch to air conditioning with recirculation rather than open windows during high pollen periods. Shield your nose and mouth with an N95 or P2 mask when mowing lawns, gardening, or handling leaf blowers, and shower promptly after outdoor exposure to remove pollen from hair and skin. Control pet allergen spread by keeping animals out of sleeping areas, bathing pets weekly if tolerated, and using HEPA vacuums and frequent grooming to reduce dander load; people with significant cat or dog allergies often see measurable reduction in symptoms by creating a pet-free bedroom and using an air purifier in sleep spaces.
Address mold and other indoor reservoirs methodically: repair leaks and water intrusions within 24–48 hours, clean visible mold with appropriate cleaners (use protective gear), and ventilate bathrooms and kitchens with exhaust fans that vent outdoors. Limit indoor plants in damp soil, store firewood outside, and use professional remediation for widespread contamination rather than DIY fixes when remediation costs exceed basic cleaning. For pest allergens such as cockroaches, seal food, fix gaps where pests enter, and consider integrated pest management plus baiting systems rather than routine spraying; these combined environmental measures often reduce symptom frequency and medication reliance for people with perennial allergic rhinitis or atopic asthma.
Fine-tune air-handling systems and daily routines for sustained benefit: choose portable HEPA units with a CADR appropriate to each living space, replace their pre-filters monthly and HEPA elements per manufacturer guidance (often every 6–12 months), and be mindful that very high-MERV filters can restrict airflow in older HVAC units—consult an HVAC professional before upgrading. Adopt a no-shoes policy at home, use doormats, and launder outer clothing after high-exposure outdoor activities to prevent bringing pollen and mold spores indoors; while traveling, select accommodations with central air-conditioning and request non-feather bedding if you have dust-mite or feather allergies.
Homeopathic Insights: Remedies and Their Effectiveness for Allergies
Overview of Homeopathy in Allergy Treatment
Classical homeopathy treats your allergy profile by matching a remedy to the totality of symptoms rather than to the allergen label; your watery eyes, burning nasal discharge, timing of symptoms (morning versus night), emotional state, and modality (what worsens or improves symptoms) guide remedy selection. Surveys show that 60–70% of patients with chronic allergic rhinitis or eczema try complementary approaches, and individualized homeopathic prescribing remains the most common model: a practitioner will repertorize your unique constellation of signs—for example, sneezing with itch at the palate, intense tearing, and relief in open air—and select a single remedy such as Allium cepa or Euphrasia accordingly.
Scientific evaluations are mixed and heterogeneous: several randomized controlled trials (sample sizes typically 300–800 participants) have reported 75–80% greater subjective symptom improvement for individualized homeopathy versus placebo on short-term measures such as total nasal symptom scores or quality-of-life scales, but systematic reviews pooling available studies note high risk of bias, variable blinding, and inconsistent outcome measures. Mechanistic explanations proposed by practitioners include immunomodulation at very low doses, reduction of histamine-mediated reactivity (remedies like Histaminum are used homeopathically), and long-term constitutional shifts after repeated individualized prescriptions.
Practical management strategies you can expect from a homeopathic pathway include acute dosing protocols (single 30C dose for a discrete allergenic exposure, repeated after 24–48 hours only if improvement is incomplete) and constitutional work for recurrent seasonal or perennial problems (200C or LM potency courses spaced over weeks). For safety, severe reactions such as airway compromise, stridor, hypotension, or progressive throat swelling require immediate conventional emergency treatment—epinephrine and emergency care should not be delayed in anaphylaxis—while homeopathy may be considered as an adjunctive, patient-directed option for milder, non‑life‑threatening allergic conditions under the supervision of a trained practitioner.
Specific Remedies for Different Allergic Reactions
Respiratory and seasonal allergic patterns commonly respond to a predictable set of remedies tailored to your symptom picture:
Allium cepa (30C) for profuse, acrid nasal discharge and burning eyes; Euphrasia (30C) for predominant eye irritation with less nasal burning and more bland nasal discharge;
Sabadilla (30C or 6C) when violent paroxysms of sneezing dominate; and Natrum muriaticum for recurrent, chronic hay fever with long-standing loss of taste or smell and watery, salt-tasting nasal discharge. You may see short-term symptom reductions of 20–30% in diary-reported nasal symptom scores within days in small trials of individualized prescribing, but patterns differ—for example, Sabadilla often suits patients whose sneezing is triggered by dust mite exposure indoors, whereas Allium cepa is frequently chosen for acute spring pollen exposures.
Cutaneous allergic reactions have a different remedy set that maps to lesion character and modalities:
- Apis mellifica (30C) for red, hot, swollen hives with stinging pain and rapid onset after insect bite or medication exposure; Urtica urens (6C–30C) for wheals that burn and sting like nettles with intense itching;
- Ledum palustre (30C) for puncture-type bites with coldness and a tendency for swelling to spread upward;
- Rhus toxicodendron (30C–200C) for itchy, weeping rashes that are worse at rest and better with movement;
- Sulphur for chronic eczema with intense burning and sleep disturbance. Data from integrative clinics often show that personalized treatment can reduce the number of hives someone experiences each week (for example, from four times a week to once) over 8 to 12 weeks, but there isn’t much controlled research, and the strength and dosing of treatments can vary.
Food and drug-related sensitivities are approached by addressing your symptom pattern rather than by “desensitizing” the specific antigen in most classical practice:
Histaminum and Arsenicum album are sometimes used for immediate histamine-type responses and food-reaction anxiety, while Apis or Ledum may be chosen for localized angioedema after a bite or medication. For pet-related allergic rhinitis, you will often see the same respiratory remedies (Allium, Euphrasia, and Natrum muriaticum) selected according to eye versus nasal predominance rather than a unique “cat” or “dog” remedy. Over-the-counter complex preparations marketed for hay fever combine low-potency remedies for broad symptom cover, but individualized single-remedy prescribing remains the method associated with the case reports and small trials that suggest benefit.
Selection, potency, and monitoring matter: you should expect your practitioner to document baseline symptom scores, set clear short-term goals (reduction in sneezing fits, night wakening, and rash area), and adjust potency—30C for acute flares, 200C for deeper constitutional interventions, and LM potencies for frequent low-dose maintenance—based on response. Combination homeopathic products and isopathic approaches for sulfite or sulfa sensitivities are used in some clinics, yet evidence is anecdotal; objective testing (skin prick, specific IgE) and avoidance strategies remain central to your safety plan, while homeopathy may be integrated as supportive care with transparent outcome tracking.
User Experiences: Success Stories and Challenges
Many people you read about or meet describe meaningful symptom relief with homeopathic care, especially for seasonal allergic rhinitis and mild eczema. Anecdotal reports commonly mention reduced sneezing, less nasal congestion, improved sleep, and a lower need for daytime antihistamines after individualized constitutional remedies; remedies frequently cited in patient accounts include Allium cepa and Euphrasia for watery, irritant conjunctivitis and nasal discharge, or Pulsatilla for changeable, mucous symptoms. Case series published by homeopathic practitioners often highlight improvements within days to weeks and reductions in over‑the‑counter medication use, which patients count as tangible benefits to quality of life during high pollen seasons or mold exposure periods.
Practical Daily Tips for Allergy Sufferers
Home Environment: Creating an Allergy-Friendly Space
Start in the room where you spend the most time: the bedroom. You can reduce dust-mite exposure by encasing your mattress and pillows in certified allergen-proof covers and washing all bedding in hot water at ≥60°C every 7 days; studies show this temperature kills >90% of dust-mite allergens. Replace feather or down pillows with synthetic, washable options and consider replacing pillows every 1–2 years if allergy testing shows ongoing reactivity. Vacuum at least once a week with a HEPA-filter vacuum (choose a model rated to capture ≥99.97% of particles ≥0.3 µm) and steam-clean or replace rugs—if you have carpets, vacuum 2–3 times weekly and plan for hard flooring in bedrooms if symptoms remain high.
Control indoor humidity to suppress both mold and dust mites: keep relative humidity between 30–50% using a dehumidifier with an auto-humidistat; many homes see measurable symptom reduction when RH is maintained below 50%. Vent bathrooms and kitchens to the outside for 10–15 minutes after showering or cooking to remove moisture spikes, and inspect basements, crawlspaces, and rooflines for leaks—address water intrusion within 48 hours to prevent mold growth. Use mold-resistant building materials where prone to dampness (e.g., cement-board backer in showers) and clean visible mold with a 1:10 bleach solution or EPA-approved fungicide following label directions; wear gloves and an N95 mask while cleaning to limit inhalation of spores.
Reduce airborne pollen and pet allergens with targeted changes: keep windows closed during high-pollen days and run central air conditioning with a MERV-11 to MERV-13 filter changed every 1–3 months depending on use, or install a portable HEPA air purifier sized to achieve 4–6 air changes per hour in your bedroom (match CADR to room volume). If you have pets, ban them from the bedroom, groom or bathe dogs weekly when possible to lower Fel d 1 levels, and store pet bedding outside the sleeping area. A case-control example: one household that added mattress encasements, switched to hard flooring in the bedroom, and ran a HEPA purifier overnight reported a >60% drop in nocturnal sneezing and nasal congestion within four weeks.
On-the-Go Strategies: Managing Allergies Away from Home
As you leave the house, carry a compact allergy kit tailored to your triggers and routines. Pack a fast-acting oral antihistamine (for example, cetirizine 10 mg or loratadine 10 mg where appropriate), a travel-size saline nasal spray (use isotonic saline ~240 mL bottles for rinses or 20–50 mL squeeze sprays), and handheld eye rinses for conjunctival exposure; check expiry dates monthly and replace medications that are out-of-date. For those with asthma or a history of anaphylaxis, always bring your inhaler and spacer, and carry an epinephrine auto‑injector—confirm the device is within its temperature storage range (typically 15–30°C) and that the needle end is protected. Use an N95 or high-efficiency mask when pollen counts exceed 50–100 grains/m³ or when entering dusty environments; N95s can reduce inhaled particle load by ~80% when fitted correctly.
- EpiPen or other epinephrine auto-injector (check expiry)
- Antihistamine tablets (non-drowsy option) and chewable if needed
- Saline nasal spray and travel eye wash
- Quick-reference allergy card (allergen list, emergency contacts, translator phrases)
- Disposable antihistamine wipes or fragrance-free wipes
- Foldable N95 mask and wrap/sunglasses to block pollen
Handle food-allergy risks with a simple routine: read ingredient labels line by line and ask restaurant staff about cross-contact—ask them to use a fresh pan or change gloves for severe allergies, and when traveling abroad, carry an allergy translation card naming your allergens in the local language. Choose dishes with single, identifiable ingredients (for example, grilled fish with steamed vegetables rather than mixed sauces or buffet items) and keep safe, non-perishable snacks in your bag to avoid reliance on uncertain food sources. Airlines and some restaurants allow pre-notified meal accommodations; requesting these ≥48 hours in advance often reduces exposure risk for shellfish, nut, egg, or dairy allergies.
Navigate public spaces with a few practical tactics that cut exposures quickly: when pollen is high, avoid outdoor exercise that increases tidal volume (running raises inhaled pollen load by several-fold), plan errands for late afternoon or after rain when counts drop, and change your clothes and shower within 30 minutes of returning indoors to remove pollen from skin and hair. On flights, take comfort in the fact that most modern commercial aircraft use HEPA filtration that removes >99% of airborne particles ≥0.3 µm from cabin air, but still wipe tray tables and armrests and request seating away from service animals if you’re highly sensitive. Any severe signs of anaphylaxis—difficulty breathing, swelling of the face or throat, persistent dizziness, or loss of consciousness—require immediate emergency attention.
The Importance of Allergy Forecasts: Staying Prepared
Understanding Allergy Levels and Their Impact
Pollen counts are typically reported as grains per cubic meter of air, and many monitoring programs group those counts into bands you can act on: low (roughly 0–30 grains/m³), moderate (about 31–90 grains/m³), high (91–150 grains/m³) and very high (above 150 grains/m³). You will notice a clear correlation between those bands and your symptoms if you track them closely; for example, people with seasonal pollen allergy often begin to experience sneezing, itchy eyes and nasal congestion once counts climb into the high range, while very high days frequently trigger full-blown hay fever and wheezing in sensitized asthmatics. Species-specific counts matter too—grass pollen peaks in late spring and early summer, birch and tree pollens spike in early spring, and ragweed surges in late summer—so a “high” grass day affects you differently than a “high” ragweed day depending on your sensitization profile.
Indoor allergen levels behave on different timescales but still interact with outdoor forecasts. Dust mite allergen levels rise when relative humidity exceeds about 50% and indoor temps sit between 20 and 25°C, meaning a damp, warm spring day can push your perennial symptoms higher even if outdoor pollen is moderate. Pet dander particles are sticky and can persist for weeks on fabrics and HVAC filters, so outdoor forecasts won’t predict those exposures—only your cleaning and filtration habits will. Mold spore counts show sharp increases after heavy rains or in basements with poor ventilation; during those post-rain windows you may see sudden spikes in sinus congestion and chronic cough that mirror the mold index rather than the pollen index.
Severity of reaction also depends on your personal threshold and comorbidities. If you have allergic asthma or atopic dermatitis, an otherwise “moderate” pollen day can precipitate ER visits or flare-ups; epidemiological data consistently show higher asthma exacerbation rates during pollen peaks and high particulate pollution episodes. You can use forecast data to quantify risk: plan higher-protection strategies (masking, HEPA filtration, pre-emptive antihistamine dose) when forecasts predict sustained counts above the high band for several consecutive days, and scale back protective steps on prolonged low-count stretches to reduce medication load and improve quality of life.
Tools and Apps for Real-Time Tracking
Several forecasting services and apps provide species-specific, hour-by-hour pollen maps that you can customize for your location. National and regional pollen networks report raw counts from certified volumetric spore traps and translate them into user-friendly indices; popular consumer tools such as Pollen.com, AccuWeather and specialized providers like BreezoMeter and the National Allergy Bureau offer push alerts for ragweed, grass and tree pollen spikes. You can set thresholds in many apps to notify you when your sensitizing allergen crosses a chosen level—use a lower threshold if you have asthma or severe food-related cross-reactivity to airborne pollens (for example, oral allergy syndrome linked to birch pollen and apple/pear exposure).
Personal and community sensors add granularity that national forecasts sometimes miss. Networks like PurpleAir provide near-real-time PM2.5 and particulate data (reported in µg/m³), which you can correlate with symptom diaries to detect pollutant-driven exacerbations; an outdoor PM2.5 reading above ~35 µg/m³ often corresponds with worse upper-airway irritation for sensitive individuals. Indoor monitors (Awair, Airthings, and Foobot) let you track humidity, VOCs and particulates so you can verify whether a high outdoor pollen day actually translates into indoor exposure—closing windows and running a HEPA purifier at speed 2–3 for 30–60 minutes after returning indoors will often cut particulate load by 50% or more, based on portable-filter performance metrics.
Integration features extend the usefulness of tracking tools: many apps now include medication reminders tied to forecast alerts, symptom-tracking modules that produce exportable reports for your ENT or allergist, and APIs to feed data into smart-home devices. For example, you can configure your smart thermostat and motorized vents to reduce intake during forecasted high pollen windows, link a pollen-alerted pre-dosing reminder to your phone 30–60 minutes before outdoor activity, and generate weekly symptom-vs-exposure charts to refine which specific pollens or indoor triggers drive your reactions.
Recommended tools to explore include Pollen.com for localized pollen calendars and species breakdowns; BreezoMeter for combined pollen and air-pollution indices with hyperlocal maps; PurpleAir for dense, community-driven particulate monitoring (real-time PM2.5); the National Allergy Bureau for certified pollen-count data; and apps from major antihistamine or ENT clinics that combine forecasts with medication reminders and symptom diaries. You can trial two complementary sources—a national forecast plus a local sensor feed—to immediately see how broad forecasts align with your immediate neighborhood exposures and tailor your preventive routine accordingly.
The Role of Healthcare Professionals in Allergy Management
When to Seek an Allergist’s Advice
You should seek an allergist immediately for any systemic reaction that involves respiratory compromise, hypotension, syncope, or loss of consciousness after exposure to a food, medication, insect sting, or other allergen; those events qualify as anaphylaxis and require epinephrine and emergency care followed by urgent specialist evaluation to confirm the trigger and prescribe an emergency action plan and epinephrine autoinjectors. For suspected drug allergies such as to amoxicillin, sulfa drugs, or NSAIDs, an allergist can perform structured skin testing, serum IgE assays where available, and supervised graded drug challenges or desensitization protocols—procedures that reduce unnecessary avoidance of first‑line antibiotics and clarify true IgE‑mediated versus delayed hypersensitivity. Any near‑miss where you needed emergency attention, required nebulized bronchodilators or systemic steroids, or developed angioedema of the tongue or throat mandates referral rather than further trial-and-error at home.
If you experience persistent upper or lower airway symptoms despite over‑the‑counter measures—nasal congestion, sneezing, itchy eyes or cough occurring more than 4 days per week and for longer than 4 weeks (the ARIA definition of persistent rhinitis)—an allergist should evaluate you for targeted testing and immunotherapy candidacy. Recurrent wheezing or two or more asthma exacerbations in a 12‑month period requiring oral steroids, ED visits, or hospitalization signals the need for specialist input to phenotype your asthma (allergic, eosinophilic, or non‑type 2) and consider controller optimization or biologic agents; randomized trials of anti‑IL‑5 and anti‑IgE biologics have demonstrated meaningful reductions in exacerbations and oral steroid use for selected patients. Chronic urticaria that persists beyond 6 weeks, daily or nearly daily hives, or angioedema without a clear trigger also benefits from allergist evaluation to pursue stepwise therapy (high‑dose antihistamines, H2 blockers, omalizumab) and targeted investigations such as thyroid autoantibodies or complement testing when indicated.
Diagnostic clarity is often the tipping point: skin prick testing (with a positive defined as a wheal at least 3 mm larger than the saline control) gives immediate answers for IgE‑mediated inhalant and food allergies but is suppressed by antihistamines, so you will typically be instructed to stop antihistamines 3–7 days beforehand depending on the agent. Serum-specific IgE testing is useful when skin testing is contraindicated or when you are taking medications that cannot be stopped; component‑resolved diagnostics can refine risk stratification for foods such as peanuts or tree nuts. When the medical history and test results don’t match, allergists conduct supervised oral food challenges or graded drug provocation tests in controlled environments to clearly confirm or rule out an allergy, which helps avoid unnecessary restrictions on diet or medication that could harm nutrition and care options.
Collaborative Care Approaches for Comprehensive Treatment
Your best outcomes often come from a coordinated team: the allergist establishes precise diagnoses and leads immunotherapy or desensitization, the primary care clinician manages routine prescriptions and comorbid conditions like allergic rhinitis or sinusitis, ENT specialists address structural issues and nasal polyps with endoscopy or surgery, pulmonologists manage severe asthma phenotypes and biologic therapy, dermatologists focus on atopic dermatitis and perform patch testing for contact allergens, and dietitians guide safe elimination diets and supervised reintroductions. Pharmacists play a vital role in medication reconciliation to identify potential culprits for suspected drug allergies and ensure appropriate epinephrine dosing; case series at large academic centers show that structured multidisciplinary clinics reduce emergency visits and improve adherence to allergy action plans by consolidating these specialties into a single care pathway.
Shared clinical pathways and data integration via electronic health records let you and your team use objective metrics to track progress: spirometry and peak flow values provide quantifiable asthma control thresholds, validated symptom scores (eg, RQLQ for rhinitis) measure quality‑of‑life gains, and serial medication‑use logs show reductions after interventions. Allergen immunotherapy typically runs 3–5 years for durable benefit; trials and meta‑analyses report symptom and medication use declines in the range of 30–50% for appropriately selected patients, so you should expect measurable improvement within 6–12 months of starting therapy. Venom immunotherapy following a systemic insect‑sting anaphylaxis reduces the risk of future systemic reactions to near zero for many patients and is an example where specialist‑led treatment changes long‑term prognosis rather than only managing symptoms.
Integrative models that incorporate complementary practitioners alongside conventional specialists can be arranged, provided there is transparent communication and a documented plan. If you elect to pursue homeopathic or other holistic treatments, coordinate this with your allergist and primary care provider so that objective monitoring continues—measures such as serial symptom scores, peak flows, specific IgE levels, and documented oral food challenges ensure that alternative approaches do not delay proven interventions. Drug desensitization, supervised immunotherapy, and emergency preparedness (epinephrine availability and training) remain standard-of-care elements that must be preserved within any collaborative plan.
Before a specialist visit, prepare a focused symptom diary, photographs of rashes or hives, dates and doses of suspected exposures, and a full medication list including OTC antihistamines and supplements; this speeds diagnostic workups such as skin testing (which gives immediate results), serum IgE assays (turnaround typically 1–2 weeks), spirometry, and CT imaging or nasal endoscopy when indicated. Expect follow‑up at intervals of 3–6 months during the initial treatment phase for titration of medications, assessment of response to immunotherapy or biologics, and adjustments to your written allergy and asthma action plans—documented plans with explicit peak‑flow thresholds and rescue steps reduce ED visits in published cohort studies and make collaborative care practical and measurable.
Summing up
On the whole you should view allergies as a spectrum of immune responses in which your body misidentifies harmless substances—pollen, dust mites, pet dander, foods, drugs, insect venoms, molds or chemicals—as threats and mounts an inflammatory reaction. That reaction can be IgE‑mediated (immediate) or non‑IgE/non‑immune mediated (delayed or irritant), and it can present as respiratory disease (sneezing, nasal congestion, cough, sore throat, seasonal or perennial rhinitis), skin involvement (rash, hives, eczema, contact dermatitis, mosquito bite reactions), gastrointestinal upset with food triggers, or systemic signs such as headache, fatigue, and, in extreme cases, anaphylaxis. You will notice patterns: pollen and ragweed trigger seasonal flares in spring and fall; dust mites and mold drive year-round symptoms; foods like milk, eggs, nuts, shellfish, soy, wheat, tomatoes, and bananas; additives like MSG or sulfites provoke immediate digestive and systemic responses; and drugs such as amoxicillin and sulfonamides can cause rashes or severe hypersensitivity. Loss of taste and smell commonly relates to nasal obstruction from inflammation but can also be a sign of viral infection or other causes, so you should assess it in the context of other symptoms.
You should use a systematic approach to identify and manage triggers and symptom patterns: a careful history, symptom diary, targeted avoidance and environmental controls (HEPA filtration, dust‑mite covers, pet management, mold remediation, and seasonal forecasting awareness) and diagnostic testing when needed (skin prick testing, serum-specific IgE, elimination diets and supervised food challenges). For respiratory and nasal symptoms you will frequently benefit from antihistamines, intranasal corticosteroids and, when appropriate, bronchodilators or inhaled steroids for lower‑airway disease; for acute skin reactions topical emollients, cold compresses or short courses of systemic therapy may be indicated. You should be alert to signs of severe reaction—difficulty breathing, throat tightness, swelling of the face or tongue, dizziness—in which case urgent medical care is warranted. Your treatment plan will often combine avoidance, symptomatic pharmacotherapy, and, where indicated, immunotherapy for long‑term modification of allergic disease; ENT and allergy specialists can guide testing and advanced interventions.
You can consider homeopathic options as part of a personalized, supportive strategy for milder, non‑life‑threatening allergy symptoms, keeping in mind that homeopathy works by matching remedy pictures to your symptom pattern rather than by targeting a specific antigen. Commonly used remedies described in homeopathic practice include
- Allium cepa for profuse watery nasal discharge with burning,
- Euphrasia when eye irritation predominates,
- Apis mellifica for swelling and stinging hives or insect‑bite reactions,
- Arsenicum album for anxious patients with burning sensations and restlessness,
- Sabadilla and Natrum muriaticum are used for common hay fever symptoms, while remedies like Nux vomica, Bryonia, or Drosera help with coughing or stomach problems caused by allergies.
For pet, pollen or mold allergies, practitioners select remedies based on the totality of your symptoms rather than the allergen label (examples above illustrate typical rubric matches). If you pursue homeopathic care, you should do so with a qualified practitioner who will individualize remedy selection and monitor response, while you continue established medical therapies for moderate or severe disease and seek emergency care for anaphylaxis or rapidly worsening respiratory symptoms.
FAQ About Allergies

Q: What are allergies and how do they develop?
A: Allergies are immune system overreactions to normally harmless substances (allergens). On first exposure, the immune system becomes sensitized and produces antibodies (often IgE); on subsequent exposures, these antibodies trigger the release of histamine and other mediators from mast cells and basophils, causing symptoms. Allergic reactions range from immediate IgE‑mediated responses (hay fever, hives, anaphylaxis) to delayed non‑IgE responses (contact dermatitis, some drug reactions).
Q: What common triggers cause allergies?
A: Frequent triggers include pollens (ragweed, tree, grass), dust mites, mold spores, animal dander (cats, dogs), insect venoms and bites (mosquito), foods (milk, egg, peanut, tree nuts, shellfish, soy, wheat, banana, apple, tomato), medications (amoxicillin, sulfa drugs), preservatives and additives (sulfites, MSG), and contact allergens (metals, latex, topical chemicals). Seasonal patterns (spring, fall) and indoor exposures (mold, dust mites, pets) strongly influence symptoms.
Q: What are typical allergy symptoms and how do they vary by type?
A: Upper airway: sneezing, runny/stuffy nose, itchy eyes and throat, watery eyes. Lower airway: cough, wheeze, chest tightness (allergic asthma). Skin: hives (urticaria), itchy rash, eczema, swelling at contact or bite sites. Gastrointestinal: vomiting, abdominal pain, and diarrhea in food allergy. Neurologic: headache from sinus congestion or allergic inflammation. Loss of taste and smell can occur from severe nasal congestion or sinusitis. Severe systemic allergy (anaphylaxis) causes throat tightness, difficulty breathing, widespread hives, dizziness, and fainting—emergency care is required.
Q: How do skin allergies, rashes, and insect bite reactions manifest, and when should I seek medical help?
A: Contact dermatitis typically causes a localized red, itchy, sometimes blistering rash at exposure sites. Urticaria presents as transient raised, itchy welts that can coalesce. Mosquito or insect‑bite allergy may cause large local swelling, prolonged itching, or hives. Seek urgent care for rapid swelling of face/lips/tongue, difficulty breathing, fainting, or widespread hives; these may signal a systemic reaction requiring immediate treatment.
Q: Can allergies cause headaches, sore throats, coughs, or a loss of taste and smell?
A: Yes. Nasal congestion and postnasal drip from allergic rhinitis can produce throat irritation, chronic coughing, sinus pressure, and headaches. Persistent congestion or sinus infection can blunt taste and smell. If loss of taste or smell is sudden or accompanied by fever, severe respiratory symptoms, or neurologic signs, seek medical evaluation to rule out infectious or neurologic causes.
Q: What conventional and holistic measures help control allergies symptoms?
A: Effective measures include allergen avoidance (pollen forecasts, HEPA filters, dust‑mite covers, pet management, and food avoidance), pharmacotherapy (oral antihistamines, intranasal corticosteroids, and short‑term decongestants), saline nasal irrigation, and allergen immunotherapy for long‑term reduction of IgE‑mediated disease. Holistic supports include environmental controls, air filtration, diet adjustments for food allergies, stress reduction; and treating coexisting sinusitis. For suspected food or drug allergies, testing and supervised re‑challenge by a specialist may be needed.
Q: What homeopathic remedies are commonly used for allergies symptoms and what safety issues apply?
A: Homeopathic practitioners commonly use remedies matched to allergies symptom patterns rather than diagnoses: for watery nasal discharge and burning eyes—Allium cepa; persistent sneezing—Sabadilla; itchy hives and swelling—Apis mellifica or Urtica urens; intensely itchy, worse at rest—Rhus toxicodendron; general histamine‑type sensitivity—Histaminum. Remedies sometimes suggested for pollen, pet or mold sensitivities include Natrum muriaticum, Arsenicum album, or specific constitutional selections. Consult a licensed medical provider for diagnosis and an experienced homeopathic practitioner for care, and do not delay conventional treatment when symptoms are severe or life‑threatening. Keep in mind that a homeopathic practitioner is first of all a medical doctor. Do not rely on individuals who believe they can recommend homeopathic treatments without medical education.
Homeopathic Treatments for Allergies in Philadelphia
At Viva Healthy Life—the holistic medical center—Dr. Tsan, an acupuncturist and homeopath, developed a special protocol for using natural remedies for allergies that stimulates the immune system of the human organism to properly tolerate airborne allergens. Both acupuncture and homeopathy are perfect solutions for different types of allergies since these methods are absolutely harmless, natural, and, more importantly, highly effective.
To schedule an appointment for a comprehensive holistic evaluation regarding your allergies, contact us at (267) 403-3085
You must be logged in to post a comment.